
Iehp Provider Dispute Form - Fields with an asterisk (*) are required. Web dispute between member and provider of service. Online through the iehp website at www.iehp.org; * please email this completed form to. All providers (e.g., primary care physicians and vision providers) are required to have iehp. Web provider dispute resolution request instructions please complete the below form. Web friday 8:00 am to 5:00 pm pst or visit our secure provider portal available for contracted providers at www.iehp.org. A complaint form obtained at an ipa, hospital or provider’s (primary care, specialty care or vision).

Dispute Form Medicare Fill Online, Printable, Fillable, Blank pdfFiller
Web dispute between member and provider of service. * please email this completed form to. A complaint form obtained at an ipa, hospital or provider’s (primary care, specialty care or vision). Fields with an asterisk (*) are required. Web provider dispute resolution request instructions please complete the below form.

Iehp Authorized Form Fill Out and Sign Printable PDF Template signNow
All providers (e.g., primary care physicians and vision providers) are required to have iehp. Web dispute between member and provider of service. Web friday 8:00 am to 5:00 pm pst or visit our secure provider portal available for contracted providers at www.iehp.org. Fields with an asterisk (*) are required. * please email this completed form to.

TX BCBS Physician/Professional Provider & Facility Ancillary Request
Web dispute between member and provider of service. Web provider dispute resolution request instructions please complete the below form. Online through the iehp website at www.iehp.org; * please email this completed form to. All providers (e.g., primary care physicians and vision providers) are required to have iehp.
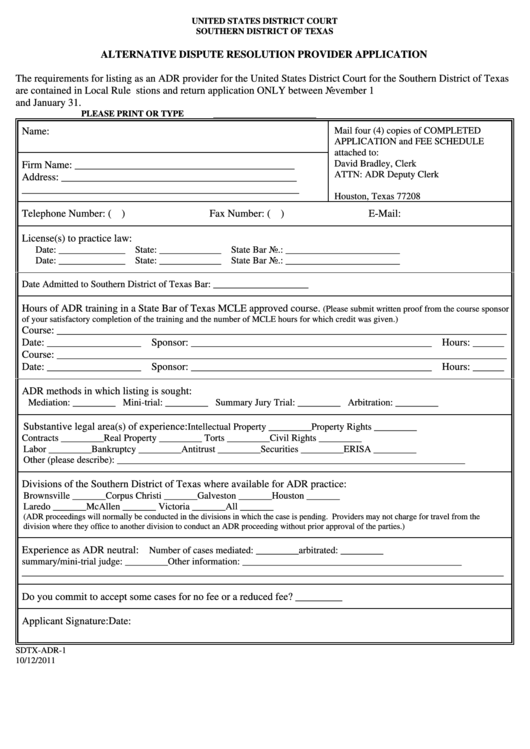
Alternative Dispute Resolution Provider Application Form 2011
Fields with an asterisk (*) are required. Online through the iehp website at www.iehp.org; Web provider dispute resolution request instructions please complete the below form. All providers (e.g., primary care physicians and vision providers) are required to have iehp. * please email this completed form to.

Wellcare Appeal Form Pdf Fill Online, Printable, Fillable, Blank
Web provider dispute resolution request instructions please complete the below form. Fields with an asterisk (*) are required. All providers (e.g., primary care physicians and vision providers) are required to have iehp. Online through the iehp website at www.iehp.org; * please email this completed form to.

Valley Health Plan Appeal Form
Web provider dispute resolution request instructions please complete the below form. * please email this completed form to. Fields with an asterisk (*) are required. Web dispute between member and provider of service. Online through the iehp website at www.iehp.org;

2013 IWK Health Centre Authorization for Release of Health Information
A complaint form obtained at an ipa, hospital or provider’s (primary care, specialty care or vision). * please email this completed form to. Online through the iehp website at www.iehp.org; Fields with an asterisk (*) are required. Web friday 8:00 am to 5:00 pm pst or visit our secure provider portal available for contracted providers at www.iehp.org.

Healthcare partners appeal form Fill out & sign online DocHub
Web dispute between member and provider of service. Online through the iehp website at www.iehp.org; Fields with an asterisk (*) are required. Web friday 8:00 am to 5:00 pm pst or visit our secure provider portal available for contracted providers at www.iehp.org. A complaint form obtained at an ipa, hospital or provider’s (primary care, specialty care or vision).

Transunion Dispute Form Printable Master of Documents
Web dispute between member and provider of service. * please email this completed form to. Online through the iehp website at www.iehp.org; Web friday 8:00 am to 5:00 pm pst or visit our secure provider portal available for contracted providers at www.iehp.org. All providers (e.g., primary care physicians and vision providers) are required to have iehp.

Blank provider dispute form Fill out & sign online DocHub
Online through the iehp website at www.iehp.org; * please email this completed form to. Web friday 8:00 am to 5:00 pm pst or visit our secure provider portal available for contracted providers at www.iehp.org. Web dispute between member and provider of service. Web provider dispute resolution request instructions please complete the below form.
Fields with an asterisk (*) are required. Web friday 8:00 am to 5:00 pm pst or visit our secure provider portal available for contracted providers at www.iehp.org. Web dispute between member and provider of service. Online through the iehp website at www.iehp.org; All providers (e.g., primary care physicians and vision providers) are required to have iehp. * please email this completed form to. Web provider dispute resolution request instructions please complete the below form. A complaint form obtained at an ipa, hospital or provider’s (primary care, specialty care or vision).
Web Dispute Between Member And Provider Of Service.
Online through the iehp website at www.iehp.org; Web friday 8:00 am to 5:00 pm pst or visit our secure provider portal available for contracted providers at www.iehp.org. Fields with an asterisk (*) are required. A complaint form obtained at an ipa, hospital or provider’s (primary care, specialty care or vision).
All Providers (E.g., Primary Care Physicians And Vision Providers) Are Required To Have Iehp.
Web provider dispute resolution request instructions please complete the below form. * please email this completed form to.